
Download PDF of this content for offline reading
This publication updates and replaces the Medical Discharge and Retirement memo of 2007.
Table of contents
- Criteria for Medical Discharge or Retirement
- Benefits of Medical Discharge or Retirement
- Counseling Considerations
- Medical Documentation
- Initiating Medical Proceedings
- Integrated Disability Evaluation System (IDES)
- Deployment of Ill and Injured Servicemembers
Attachment: IDES Timeline Chart graphic
Introduction
Attorneys and counselors are seeing increasing numbers of soldiers and sailors with physical and emotional injuries and illnesses, many resulting from the wars in Iraq and Afghanistan. The military’s handling of various medical conditions is often affected by the demands on commanders to fill their rosters for deployments, by lack of training or understanding of the regulations, by pressure on medical personnel to return patients to duty, by the current trend of “downsizing,” and sometimes by military cultural biases that perceive ill or injured servicemembers as weaklings or malingerers. As a result, many who qualify for medical discharge or retirement are retained in the military, discharged for lesser psychiatric or physical problems that do not warrant benefits or, worse, for misconduct based on the symptoms of their illness. As a result of pressure from investigative reporting in the mainstream press and political pressure from Members of Congress, some new policies have been put in place to counter these problems.
Counselors and attorneys can play an essential role in helping servicemembers receive proper medical treatment, and medical discharge or retirement when appropriate. Advocates can also ensure that members’ rights are protected in this process, and that under-diagnosis or lack of diagnosis does not result in loss of military and veterans benefits.
Criteria for Medical Discharge or Retirement
Authority
Department of Defense (DoD) instructions and service regulations list conditions which may warrant medical discharge or retirement. DoD Instruction 1332.38 is the controlling regulation. It lists, in Enclosure 4, medical conditions that generally warrant referral for medical discharge/retirement proceedings. The service regulations include Army Regulation (AR) 40-501, chapter 3; Secretary of the Navy Instruction (SECNAVINST) 1850.4E, Enclosure 8, which covers Navy and Marine Corps personnel; and Air Force Instruction (AFI) 36-2902.
Medical Conditions
In General
“Any condition that appears to significantly interfere with performance of duties appropriate to a servicemember’s office, grade, rank or rating will be considered.” (DoD 1332.38, Encl. 4.1.3) Most conditions listed in the regulations are not automatically disqualifying. Rather, discharge or retirement usually depends on the conditions’ severity, amenability to treatment and, in particular, interference with performance of duties. These factors are often stated in the medical standards. For example, tendon transplantation warrants referral for discharge/retirement proceedings “[i]f restoration of function is not sufficient to adequately perform the preponderance of duties required.” (DoD 1332.38, Encl. 4.2.) These conditions render members medically “unfit” for service.
In the Line of Duty
Conditions need not be related to combat or incurred while performing regular military duties to warrant medical discharge or retirement and benefits. They are considered to have occurred “in the line of duty” if they arose (or were aggravated) after entry onto active duty, were not the result of misconduct or willful negligence, and were not incurred during a period of unauthorized absence (UA or AWOL).
Preexisting or Arising Early in Service
Many medical conditions which appear in the first few months of active service are presumed to be preexisting (this co-exists with a legal presumption that members were in good health upon entry). Such early medical problems are sometimes referred to a medical evaluation board, but may then result in administrative discharge for erroneous enlistment or in medical discharge without full proceedings to determine disability status. Pre-existing conditions that are aggravated by military service should not fall into this category but rather treated as a medical condition that warrants evaluation for possible medical discharge.
Discharge is permitted in the first few months for conditions which do not warrant medical discharge, but would have prevented enlistment under the less stringent enlistment medical standards. These are found in Department of Defense Directive 6130.3, Physical Standards for Appointment, Enlistment and Induction, and in AR 40-501, chapter 2, which provides guidance for pre-enlistment physical examinations for all of the services. Erroneous enlistment discharge proceedings or abbreviated medical proceedings may be used for these conditions. See, for example, AR 635-200, Section 5-11, “Separation of persons who did not meet procurement medical fitness standards.”
After the first few months of service, pre-existing conditions that are not aggravated by military service result in medical discharge without benefits (unless the member has served eight years), as do conditions found not to be in the line of duty.
Administrative discharges for medical conditions
Medical problems arising during the first 180 days of active service may lead to administrative discharge for Entry Level Performance and Conduct, with simplified administrative procedures and no requirement of a medical evaluation board. The discharge is based instead on command determinations that the members are not qualified for further military service by reason of unsatisfactory performance or conduct. In theory, this category is used for conditions not serious enough to warrant medical discharge or retirement for a condition incurred in the line of duty. However, counselors and attorneys should be aware that conditions warranting medical discharge or retirement are sometimes wrongly handled under this category.
A number of medical conditions not considered serious enough to warrant disability proceedings may result in involuntary administrative discharge at any time. Most of these are set out in DoD 1332.38, Encl. 5. The governing regulation on enlisted separations, DoD Directive 1332.14, Encl. 3, part 3.a.(8) lists some “other designated physical or mental conditions” which may warrant administrative discharge, but leaves the services free to expand the list. Applicable service regulations include AR 635-200, Chapter 5, sections 5-13 and 5-17; Naval Military Personnel Manual (MILPERSMAN) sections 1910-120 and 1910-122; Marine Corps Separation and Retirement Manual (MARCORSEPMAN) section 6203; and AFI 36-3208, section 5.11. Criteria for this discharge vary among the services, though all branches include psychiatric conditions called personality disorders, and most include physical problems such as airsickness or seasickness, sleepwalking, enuresis and the like. Some services have added learning disorders and adjustment disorders to these lists. Here, too, conditions warranting medical discharge or retirement are sometimes shoehorned into this category by mis- or under-diagnosis.
Benefits of Medical Discharge or Retirement
Military Benefits vs. Veterans Administration Benefits in General
Medical discharge or retirement can mean important medical and financial benefits for veterans.
Some of these parallel the Department of Veteran’s Affairs (VA) medical benefits, although medical retirement offers a wider range of benefits and, for those who have a fairly long time in the service, higher disability compensation. For some veterans, retirement benefits – such as the ability to choose between military medical care and VA medical care, family medical care, use of base commissaries and the like – may be important considerations in seeking medical retirement.
Another difference between the DoD and VA benefits arises because the military system bases disability pay on length of service. Therefore, shorter-term servicemembers usually receive a higher benefit from the VA.
The services’ Physical Evaluation Board Liaison Officers (called PEBLOs) may be very helpful in calculating financial and other benefits of medical discharge or retirement, and comparing these with VA benefits. Rod Powers’ article on medical discharge and retirement, available at usmilitary.about.com, contains an excellent summary of disability payments.
Military Medical Discharge vs. Retirement
What is required for medical retirement rather than discharge?
Although the military uses its own medical standards to determine whether members should be processed for medical discharge/retirement, it relies on the Department of Veteran’s Affairs (VA) Schedule for Rating Disabilities (38 Code of Federal Regulations, Part 4) to determine the degree of disability and accompanying compensation. Under the military’s new Integrated Disability Evaluation System (IDES), the military accepts VA rating determinations on all conditions the military considers unfitting. (VA may also rate conditions that are not unfitting, for which the military will not provide disability compensation. For example, the services will accept a VA rating of 30% for major depression, but ignore the VA’s rating of 10% for scarring, which is not considered unfitting.)
The military normally provides no benefits for those found medically unfit from conditions which existed prior to entry onto active duty, unless the conditions were aggravated in the military; then the services will rate and compensate for the aggravation. However, members with more than eight years of active service should receive severance pay or disability retirement pay for all pre-existing conditions as if their conditions were incurred on active duty.
Those whose illness or injury occurred during unauthorized absences (AWOLs or UAs) or as the result of their own misconduct or willful negligence, will be medically discharged but receive no compensation. These conditions are described as “not in the line of duty.”
Line of duty conditions considered less severe may receive either no compensation or a lump-sum payment from the military, leaving the servicemember free to seek compensation from the VA. Those considered more severe result in medical retirement with monthly disability pension payments and a choice of care and administration of benefits through the military or the VA, as well as other retirement benefits. Needless to say, these determinations may be critical for members whose illness or injuries may have long-term effects on their livelihood.
Members who are found medically unfit from conditions incurred in the line of duty will receive medical discharge with a lump-sum severance payment if their disability rating is determined to be less than 30% and they have not served for 20 years. Severance pay is calculated at two months basic pay times their years of military service (not to exceed 24 months basic pay). On discharge, these individuals can apply to the VA for medical care and disability compensation; however, the amount of money received in severance pay is deducted from compensation later received from the VA.
Servicemembers with conditions incurred in the line of duty who receive military disability ratings of 30% or more are retired from the service. Depending on the stability of their condition, they may be placed on the Permanent Disability Retirement List (PDL) or the Temporary Disability Retirement List (TDRL). Medical retirees in the latter category are reevaluated at 18-month intervals for five years. If their conditions do not change within that period, they are then transferred to the PDL. If any of the reevaluations show significant improvement, they may be discharged or (rarely) returned to military service; if reevaluations show stability, they may be moved to the PDL at that time.
Calculations of disability retirement pay are based on “retired base pay.” For those who entered military service after September 8, 1980, retired base pay is the average of the highest 36 months of basic pay during their service. For those who entered before that date, retired base pay is the highest basic pay they received while in the service. Disability payment is then determined from the higher of two computations: the disability rating times the retired pay base, or 2.5 times years of service times the retired pay base. TDRL members will not receive less than 50% of retired base pay. (Separate calculations are used for reservists.)
Eligibility for VA Medical Benefits
Veterans may ask the VA to make its own determination about eligibility for VA benefits. Military medical determinations are given considerable weight by the VA, but the VA should consider its own evaluations and any additional evidence provided by veterans. In addition, the VA will sometimes provide benefits for those whose illnesses or injuries are not deemed “service connected” under VA standards.
Counseling Considerations
Many medical discharge cases begin when clients come to counselors or attorneys with questions about medical problems or discharges in general. In initial counseling for those seeking any discharge, it is wise to explore the possibility of medical discharge or retirement. All too often soldiers live with medical conditions that qualify for discharge/retirement because they have given up trying to get help or believe that pointing out medical problems would be considered admissions of weakness and subject them to ridicule. Psychiatric problems, in particular, are often unmentioned. Counselors and attorneys can ask clients to read through the list of medical conditions warranting discharge or ask them generally about all of their medical problems and compare those to the medical standards.
Nothing in the regulations prevents service members from pursuing medical discharge and other discharges at the same time. Medical discharges and, for example, hardship discharges may easily be raised simultaneously. Some counselors and attorneys make an exception for conscientious objection discharge, where regulations urge commands to look for ulterior motives or other reasons the CO applicant might seek discharge. Some also warn clients about combining discharges when the members’ honesty about symptoms may be critical to diagnosis and the other discharge rests on the members’ subjective statements and honesty as well.
Many servicemembers who received medical treatment or had medical problems prior to enlistment were encouraged by their recruiters to lie about the conditions. In other cases, the recruits themselves may have denied health problems to ensure enlistment. Pre-service problems may come up in discussion with military doctors or may provide important documentation for members whose medical problems are otherwise difficult to prove. Members alleged to have concealed medical information may face administrative discharge for fraudulent enlistment or erroneous enlistment. Under current discharge regulations for the Navy, Marine Corps and Air Force, these discharges must be honorable, general under honorable conditions, or entry level (uncharacterized); they cannot be characterized as other than honorable. The Army regulation permits other than honorable discharges. Occasionally servicemembers are threatened with prosecution for fraudulent enlistment; the authors of this article have never seen such a prosecution for medical concealment, but the mere threat can be intimidating. These issues should be discussed with clients, so that they are not caught unaware by threats and can make an educated decision about the possibility of discharge documents showing discharge for fraudulent enlistment.
Medical Discharge/Retirement and Administrative Separation
Medical separation takes priority over most administrative discharges. For example, unsatisfactory performance or weight control discharges should be halted if medical problems are referred for disability proceedings; soldiers diagnosed with personality disorders warranting administrative discharge and with severe depression or PTSD warranting medical retirement should be medically processed. Unfortunately, misdiagnoses and commands’ desires to rid themselves of unproductive members have often led to administrative discharges where medical proceedings are appropriate.
Medical separation normally does not take priority over discharges which warrant other than honorable characterization or over disciplinary action and punitive discharge. Before deciding on a medical discharge, counselors or attorneys should inquire about pending or possible involuntary discharges, investigations or disciplinary actions. Discharges in which an other than honorable discharge may be authorized (even if not recommended in the individual case) generally take precedence over medical proceedings (DoD 1332.38, Encl. 3.2.4.3). Similarly, pending approved unsuspended punitive discharges or dismissals preempt medical proceedings. (DoD 1332.38, Encl. 3.2.4.2) However, DODI 1332.38 does direct individual services to provide for military members’ referral to the disability system if they have medical impairments or extenuating circumstances that are cause of the conduct for which they are being separated (Encl. 3.2.4.4; see also AR 635-200, paragraph 15-16 b.). Counselors contacted by military members who face separation under these conditions should inquire about health concerns that may have contributed to the conduct for which they are being separated.
Unless the case can be made for a causal relationship between the conduct and a medical impairment, medical discharge processing is normally suspended pending such administrative discharge proceedings or disciplinary proceedings, then dropped altogether if the other proceedings result in discharge in the Navy, Marine Corps and Air Force; the Army proceeds with medical evaluation boards and gives the administrative separation authority the option of medical discharge/retirement in appropriate cases. All too often, symptoms of medical problems are viewed by commands as misconduct warranting administrative separation with an other than honorable discharge. Medical problems may be raised as mitigation in discharge or court-martial proceedings to avoid other than honorable or punitive discharges or even to seek referral to the disability system. Such mitigation may result in retention in the service, leaving the way open for later medical discharge or retirement; or in a general or honorable discharge permitting VA medical care and benefits.
An amendment to the 2010 National Defense Authorization Act included added procedures to screen for PTSD and TBI in some servicemembers who are facing OTH administrative discharge. DoD incorporated these changes first through Directive-Type Memorandum 10-022 and then through DoD Instruction 1332.14. This instruction requires a medical examination for TBI and PTSD prior to separation if servicemembers are being administratively separated under OTH conditions, were “deployed overseas to a contingency operation [formerly called combat areas] during the previous 24 months,” and are either “diagnosed by a physician, clinical psychologist, or psychiatrist as experiencing PTSD or TBI,” or the servicemembers have a “reasonable allegation” of PTSD or TBI.
If servicemembers meet these requirements, they “must receive” a medical exam to screen for PTSD and TBI. The purpose of the exam is not only to diagnose the condition, but also to determine whether PTSD or TBI is responsible for or mitigates some of the circumstances of the members’ OTH and –if so – potentially change the character of discharge or basis of separation. Servicemembers who qualify for this examination will not be separated until the appropriate authorities, as determined by the Secretary concerned, have reviewed the results of the examination.
However, this policy does not change the fact that OTH discharges take precedence over medical discharges/retirement. Even if DoD 1332.14 results in a change in characterization of the discharge, servicemembers may still not be entitled to medical retirement, even if their PTSD or TBI is disabling. In such situations, some servicemembers may be able to fall back on DODI 1332.38 Encl. 3.2.4.4. While this instruction does not require commands to seek an evaluation for PTSD or TBI for servicemembers, counselors can help servicemembers acquire such an evaluation through civilian channels, if necessary, and help push for referral into the disability system if they can demonstrate that their medical impairment was the cause of the conduct for which they are being separated.
(For more information about administrative discharges, and the procedures used to challenge them, see MLTF’s memo, “Representing Servicemembers in Involuntary Discharge Proceedings.”)
Medical Documentation
Servicemembers may consult attorneys or counselors after diagnoses of their problems by military or civilian doctors. More often, medical problems have not been diagnosed by the military, servicemembers have difficulty accessing military doctors, or members feel they have been misdiagnosed by military doctors. In these cases, it is extremely helpful to begin by sending clients to civilian physicians – specialists if possible. While the military is not bound by civilian medical reports, they can be persuasive. Submission of civilian reports giving specific diagnoses and descriptions of severity can help clients gain access to military doctors and can help those doctors in coming to correct conclusions.
If the clients already have diagnoses and are confident of their accuracy, existing records may suffice, though even here civilian reports may be valuable in lending additional emphasis to the severity of the condition.
In all medical cases, it is useful to obtain copies of all military medical records, and any relevant civilian medical records, at the outset, and for attorneys or counselors to review the records with the clients. It is worth noting that clients are not always aware of helpful or harmful entries in their military medical records, including diagnoses other than those mentioned to patients. Soldiers who have heard “you’re depressed” from their military doctors may find that they have been diagnosed with adjustment disorders and/or personality disorders rather than depression. The diagnoses of record can be compared with the conditions warranting medical discharge/retirement in the service regulation. In many cases the specific condition will be listed; if not, a civilian health care expert can look for the presence of similar conditions with similar effects, severity and prognosis. The DVA rating schedule can be used to determine symptoms or standards used to measure severity.
Initiating Medical Proceedings
In some cases, the existence of a medical condition by itself is enough to lead commands to refer members to sick call and lead commanders (in the Army) or military doctors to initiate medical discharge proceedings of their own accord. Here it may be sufficient for clients to present themselves for evaluation. Often, however, commands or medical personnel (usually medics or corpsmen) make it difficult to see military physicians. And military doctors may fail to recognize problems, may delay in making diagnoses, or may make efforts at treatment before deciding whether conditions require discharge. In these cases, outside assistance may be important at the outset, and service differences are significant.
In the Army, unlike the other services, disability proceedings often begin with a referral by the commanding officer, specifically asking that a medical evaluation be conducted (AR 635-40, Section II, Initiation of Medical Evaluation, paragraph 4-8). The other services are less concerned about referrals by commands. Informally, treating physicians, particularly specialists, often initiate the process for medical evaluation boards (MEBs). In all services, heads of medical treatment facilities may request MEBs, as may the service’s medical headquarters. Thus, if doctors fail to act on their own, counsel in Army cases may wish to address a letter to the command, providing documentation of the condition and requesting medical discharge. The same letter could, of course, be directed to the head of the medical treatment facility or the service’s Surgeon General. In other services, this request is better addressed to the treating doctor, the head of the treating facility, or medical headquarters.
The role of Army commands in medical processing is also made confusing by the Army’s heavy reliance on its separate medical “profiling” system. Here doctors are asked to evaluate members’ availability for full duty, deployment, etc., and to note any restrictions on duty; except where base policies require compliance with profiles, commanders have sole discretion to decide how or whether to act on the profile presented by doctors. However, they “are responsible for … the assignment of the individual to military duties commensurate with the individual’s physical profile and recorded assignment limitations (AR 40-501, Paragraph 7-12.a). If Army commanders decide not to act on a “P4” profile for PTSD, which should normally preclude deployment, Army doctors can still initiate medical discharge/retirement proceedings. Unfortunately, many commands, soldiers and even Army doctors tend to assume that commands have greater authority than the regulations allow, and civilian advocates may need to remind both commands and doctors of the requirements of the regulations.
Members with medical problems have little or no access to legal help through the military in the early stages of their cases. Military counsel is not normally available to soldiers who are having problems gaining access to doctors, feel they have been badly treated in the medical system, or believe that medical evaluation boards should have been prepared long ago. Under the IDES system, members should be able to consult with military attorneys when MEB proceedings have been initiated or are contemplated. In addition, non-attorney benefits counselors, called physical evaluation board liaison officers (PEBLOs), meet with servicemembers to explain the discharge/retirement process and the members’ rights during MEB processing. (PEBLOs play an important role in providing information and processing cases; it is always helpful for members to develop good relationships with their PEBLOs.)
Military counselors or attorneys can play an essential role in the early stages of cases. Members are generally not familiar with the medical standards governing discharge, and may be misled by over-worked corpsmen, medics or doctors, as well as unsympathetic commands. Few have any idea of the criteria which might make the difference between a medical discharge without disability benefits for a pre-existing condition or medical retirement with disability benefits. Full discussion of grounds for discharge/retirement and disability evaluation procedures can provide critical assistance.
As noted above, many soldiers and sailors find it difficult to gain access to military doctors, who are frequently overworked and sometimes more sympathetic to commands’ needs than patients’ medical problems. In many areas, non-physicians serve as gatekeepers; they and medical officers serving in the field may be the most likely to under-diagnose medical and psychiatric problems that should warrant referral to a specialist or even emergency treatment. Advocates can help members move through this sometimes unfriendly system by bringing pressure on commands, medical treatment facilities or medical headquarters, or by enlisting the assistance of civilian physicians to document problems and urge evaluation and treatment.
The right to medical evaluation and care is not discussed much in military regulations, though it is assumed to be a basic right. Some help can be found in DoD Instruction 6000.14, DoD Patient Bill of Rights and Responsibilities in the Military Health System (MHS), enacted in keeping with the civilian concept of patients’ bills of rights. Aimed at military treatment facilities rather than commands, it states that “[p]atients have the right to quality care and treatment that is consistent with available resources and generally accepted standards, including access to specialty care and to pain assessment and management.” (DoD 6000.14, Encl. 2, Part 1.) The Instruction also describes complaint procedures available to patients. (Encl. 2, Part 1.g. and Encl. 3, Part 2.g.)
With problems that are difficult to measure, including some psychiatric conditions and physical conditions which manifest in such elusive symptoms as back pain or headaches, civilian documentation and pressure from an advocate may be important in ensuring that problems are taken seriously. Reports from civilian doctors are particularly helpful, making it difficult for commands and military doctors to ignore the condition, and providing documentation for complaints if they do so.
Part of this process involves helping soldiers or sailors to be effective patients. Many servicemembers downplay medical problems to avoid ridicule or harassment. They should receive an explanation of the value of full reporting of problems and of repeated visits to sick call or their individual doctors whenever symptoms arise. Most counselors and attorneys encourage their clients not to present as members wanting their rights or wanting discharge, but rather as patients wanting help with problems. Military doctors are often happier if they are the first to conclude that medical discharge/retirement is warranted.
Members also need to be warned that military medical records are not confidential, and that information they provide to military doctors or mental health professionals can be repeated to their commands. Information given to doctors about members’ violation of regulations may lead to involuntary administrative discharge or disciplinary action, in some case resulting in loss of medical benefits.
If access to physicians is denied, sometimes informal appeal to the commanding officer by members or their advocates will make access easier. Formal letters from counsel requesting medical evaluation sometimes provide the necessary impetus. In other cases, formal complaints under UCMJ Article 138 are necessary. Parallel letters and complaints can be made to the commander of the military treatment facility involved and to the surgeon general of the service. Some counselors and attorneys have found ombudsmen and patient advocates at military medical facilities to be helpful, as well.
The regulations offer little guidance on time frames for medical evaluation and treatment. When cases stall, and referrals to MEBs are not forthcoming, counselors or attorneys may need to recommend a reasonable time and demand that the service justify any delay beyond that point. The issue of how long the service can take before responding to certain requests should be judged under a reasonableness standard. Where members have given the military the opportunity to grant the relief requested or to rectify any unwarranted denial of a request for relief, and have submitted appeals to the secretary of the service, administrative remedies have been exhausted for purposes of federal court intervention. The military should not be able to avoid the consequences of unreasonable delays by transferring members to a war zone and away from the assistance of their attorneys.
When in-service remedies have been exhausted, attorneys may go into federal district court to challenge any denial deemed arbitrary and capricious or without basis in fact. GIs may prevail on a writ of habeas corpus or writ of mandamus in such a forum if they have provided a prima facie case warranting medical discharge or retirement, and the military has failed to disprove the existence of the medical condition identified in the prima facie case.
Integrated Disability Evaluation System
In General
The Integrated Disability Evaluation System (IDES) is a relatively new system which combines military and Veterans Administration (VA) evaluations and rating decisions. It is comprised of three main parts and processes: 1) the Medical Evaluation Board (MEB), 2) the Physical Evaluation Board (PEB), and 3) the VA disability rating system. Generally, the MEB determines the medical conditions of the service member and the PEB determines if the servicemember is “fit for duty” (continued service). For those determined to be “unfit”, the PEB applies a disability rating provided by the VA Disability Rating Activity Site (VA-DRAS). The “Integrated” concept describes a change in procedures implemented during 2010-2012 whereby VA certified doctors perform medical evaluations used by the military’s MEB and PEB and for the VA disability rating. This allows the VA to calculate a disability benefit for service members before they are discharged and to begin VA benefits within 30 days of the servicemember’s discharge from active or reserve status. Previously, the VA performed its own medical evaluations after veterans were discharged and then assigned a VA disability rating and processed the VA disability benefits. The integration of the military and veterans disability evaluation systems was meant to streamline the medical evaluation process and reduce the amount of time between discharge from the service and commencement of VA benefits.
Although the commencement of VA disability benefits may be earlier than under the old system, the MEB/PEB process is taking longer than it did under the old system and longer than the goals set for the IDES program. There are many factors affecting the length of time needed to get through the entire IDES process including, but not limited to, lack of adequate staffing, training of personnel on the new system, the number of medical conditions of the servicemember, and an increase in the number of servicemembers in the system. Servicemembers should expect the process to take nearly one year and possibly longer.
Note: Servicemembers whose cases were initiated under the legacy DES process will not enter IDES. There may be cases that fall into this category because IDES was implemented over a period of time and not all military installations are IDES sites.
It should be noted that military disability ratings and VA ratings may differ because there are some conditions the VA considers and rates as disabilities that the military does not consider unfitting. These differences are described in DoD Instruction 1332.39. One example is the physical appearance of scarring or other disfigurement that does not interfere with functioning.
Governing Federal Statute, DoD Directives and Instructions, and Service Regulations
The Integrated Disability Evaluation System and the process for medical discharge and retirement are governed by statute. (10 USC 1201-1221.) Detailed IDES procedures are set forth in Directive-Type Memorandum (DTM) 11-015, which will be incorporated in February 2014 into DoD Instruction 1332.38, Physical Disability Evaluation. The authority and policy of the DoD Disability Evaluation System is established by DoD Directive1332.18, Separation or Retirement for Physical Disability, which appears to be in need of updating for the changes resulting from IDES. Instructions for rating disabilities of “unfit” service members found to be eligible for medical discharge or retirement are found in DoD Instruction 1332.39, Application of Veterans Administration Schedule for Rating Disabilities.
Service department specific regulations are found in SECNAVINST 1850.4E (the Navy Manual of the Medical Department, or MEDMAN, is also helpful), AR 635-40, and AFI 36-3212. Be aware that these regulations may or may not already be updated for changes resulting from the implementation of IDES through DTM 11-015. There are variations between services, so it is important to work with individual service regulations as well as the DoD Instructions and Directive. In addition, there is a significant body of case law on the disability system and the rights of those considered for medical discharge or retirement; unfortunately, almost all of the cases, like the regulations, deal with individuals who have already entered the system through a medical evaluation board.
Legal Representation
Service members are entitled to legal representation provided by the Military Department at no charge, private counsel retained at the servicemembers’ expense, or a VA-accredited representative during all steps of the PEB determinations. A VA-accredited representative or attorney may represent the servicemember before the VA during the pre-separation portion of the IDES where servicemembers receive their VA Disability Rating and benefit amount. (See DTM 11-015, Attach 2, Para 4 (j), (k) and Append 1 to Attach 4, Para 1a.)
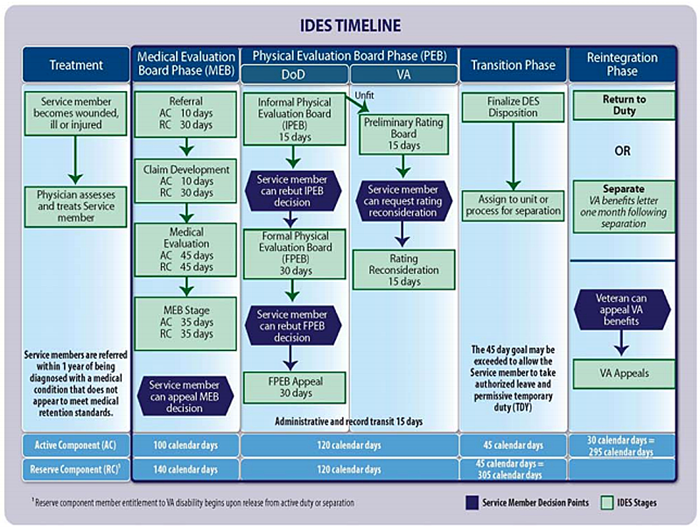
Process Overview and Target Timeline
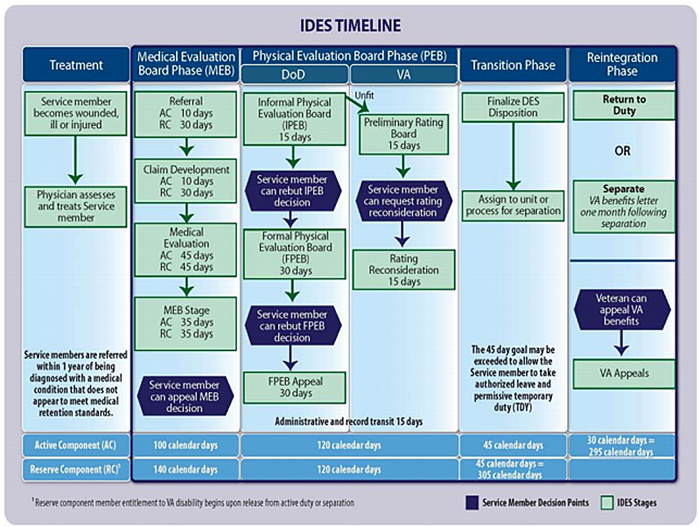
Click image for larger version
This graphic was created by IDES program administrators and includes the target number of days for each step in the process. The dark hexagons identify points in the process where servicemembers may rebut or appeal decisions.
Source – DTM-11-015, Attachment 9
Click on image, or see Appendix of PDF version for larger version of timeline.
Key Personnel, Their Duties and the IDES Process
DTM-11-015, at attachment 3, sets out the principal personnel and agencies in the IDES system. These include:
- Military medical care provider: works in a military treatment facility (MTF) and makes the referral to IDES.
- MTF patient administrator: receives the IDES referral from the medical care provider and assigns a Physical Evaluation Board Liaison Officer (PEBLO).
- PEBLO: informs servicemembers of the IDES process, assembles DES case files, enrolls the servicemembers in the Veterans Tracking Application (VTA), and refers the servicemembers to a VA Military Service Coordinator (MSC).
- VA MSC: informs servicemembers of the IDES process and requests that qualified medical examiners perform the medical examinations required to adjudicate disability claims.
- Qualified medical examiners: are medical professionals who have been trained on IDES and how to report the medical information needed to make fitness for duty evaluations and disability ratings using standardized forms. They perform the medical examinations required to adjudicate the fitness for duty determination and disability rating determinations.
- VA MSC: provides the completed medical examination results to the PEBLO and the VA Disability Evaluation System Rating Activity Site (D-RAS).
- PEBLO: incorporates the medical examination results in the IDES case file and provides it to the Medical Evaluation Board (MEB) convening authority.
- MEB: consists of two or three physicians convened by the MTF commander. MEB members receive the case file from the PEBLO, consult, prepare a narrative medical report and render a decision on whether the servicemembers should be entered into the disability system. Servicemembers may file a rebuttal to the MEB report, in which case the MEB will evaluate the rebuttal and make a response.
- PEBLO: receives the MEB report from the MEB and provides copies to servicemembers along with the VA medical examination results. If the MEB did not return the servicemembers to duty, the PEBLO forwards the case file to the Informal Physical Evaluation Board (IPEB).
- VA D-RAS: prepares and provides the proposed disability ratings, performs reconsideration of the proposed ratings when requested by servicemembers, and forwards to the Informal Physical Evaluation Board (IPEB).
- IPEB: makes a determination of fitness or unfitness on each medical condition (adjudicates the servicemember’s case) from the complete MEB case file and forwards the findings to the PEB administration staff. Applies the disability ratings from the D-RAS to the unfitting conditions and publishes the disposition recommendation (retention, discharge, retirement). The PEBLO provides the PEB report to the servicemembers, who may submit a request for reconsideration and, if necessary, request a Formal PEB (FPEB) if they disagree with any of the findings of the PEB. The PEB has discretion in granting servicemembers’ request for a FPEB when the IPEB has found fitness for all conditions.
- FPEB: provides a hearing and considers servicemembers’ rebuttals of issues pertaining to the fitness of conditions for service and the ratings assigned to unfitting conditions. If servicemembers appeals a FPEB decision, it is sent to the military department for disposition.
Referral to IDES
Cases begin formally when a military medical care provider determines that servicemembers’ injuries or illnesses are likely to render them unfit for continued military service either by virtue of the seriousness of the condition or the lack of improvement after one year of treatment. The medical care provider consults with the servicemembers’ commander and obtains approval from the MEB convening authority before referring to IDES. A military treatment facility (MTF) patient administrator assigns a PEBLO who explains the entire process to the servicemember.
Medical Evaluation Board (MEB)
Military medical providers, usually a specialist and two other medical personnel, prepare an MEB report (sometimes called a “medical board” or “med board”). MEBs do not formally convene, and they offer members no formal opportunity to testify or present evidence. Rather, their reports are based on the observations and opinions of the board members after reviewing the IDES case file, which includes the servicemembers’ medical history and results of the examinations by the IDES qualified medical examiners. The regulations set out detailed requirements for MEB reports, including types of testing required for some specific medical conditions. The reports include diagnoses, origin and history of the conditions and descriptions of treatment. The reports state whether the conditions are cause for referral into the physical evaluation board (PEB), but should not offer opinions on whether or not members are medically fit or unfit for duty. These boards do not make recommendations for discharge or retirement, or suggest any percentage of disability.
Any MEB listing a psychiatric diagnosis must contain a thorough psychiatric evaluation and include the signature of at least one psychiatrist or psychologist with a doctorate degree in psychology. (DTM-11-015, Appendix 5 to Attachment 4, page 23.)
Command Non-medical Assessment
Under current regulations, MEB reports must be accompanied by non-medical assessments prepared by the members’ command, discussing the effects of conditions on performance of duties. (DTM-11-015, Attachment 10, page 54.) This is the only formal role commands have in the process once the disability proceedings have been initiated. These assessments are quite significant, however, since the impact of conditions on members’ ability to perform duties is an important factor in determining unfitness and disability percentage. This makes it essential that servicemembers communicate symptoms and their impact on duties to the command while seeking medical attention.
Getting All Symptoms into the Record
Servicemembers may claim any conditions not initially reported by their referring physician by completing Section 2 of VA Form 21-0819 and DD form 2807-I Report of Medical History. If servicemembers do not let their medical personnel know about symptoms, a condition may be overlooked.
The down side is that, the more symptoms servicemembers present, the more medical evaluation needs to be performed and the longer the process takes. Many servicemembers are reticent to say anything that might make the process take longer. It is difficult to come back to the VA later and report symptoms that are not already in the record and claim the symptoms as service connected. Servicemembers may also fear that signing the VA and DD forms referenced in the above paragraph may be used against them because they include information about the origin, incurrence or aggravation of their disease or injury, which in some cases may reveal conduct in violation of regulations. However, Title 10, Chapter 61, Section 1219 of the US Code prohibits the use of such information against the best interests of the servicemember. (DTM-11-015, Appendix 1 to Attachment 4, page. 13. Note, though that information contained in unsigned medical records is sometimes used in administrative and disciplinary proceedings.)
Another opportunity to get symptoms into the record occurs during the physical exam for discharge. Whether a physical exam for discharge takes place depends upon how long it has been since the servicemembers’ last medical exam. If a condition found in a discharge examination is serious enough, the examiner may refer the servicemembers back to the MEB. This is another area where it is not possible to know what will happen until servicemembers are there. The safest counseling approach is to make sure servicemembers understand it is in their interest to bring all symptoms to the attention of the medical examiner during the IDES process if not earlier.
Line of Duty Investigations
Line of duty investigations may be required in cases of accident or where there is any concern that conditions may have resulted from members’ misconduct or willful negligence, as well as in certain situations involving reservists. (DoDI 1332.38, Encl. 3.4.4). In some cases, as when there is concern about misconduct or willful negligence, these may be formal investigations, not simply prepared by commands, but by appointed investigating officers, frequently military attorneys. Command members may be interviewed as part of formal investigations, and command attitudes may thus affect a basic determinant of eligibility for benefits.
Rebuttal by Service Member
Members must be given a copy of the signed MEB report including VA disability evaluation results and may submit a rebuttal if they disagree with any of the medical findings within the report or the MEB’s decision to refer them to the PEB. In some cases, PEBLOs and other personnel will pressure members to sign the MEB report and waive the right to rebuttal on the spot. However, it is always wisest to have attorneys or counselors review the reports and discuss them with clients before deciding on the value of a rebuttal. Even small errors regarding symptoms, severity, origin or effect on duties may affect the outcome. If rebuttal is appropriate, it offers an opportunity to provide additional documentation of the medical condition discussed in the report, or other medical conditions omitted from the report. Service members should be counseled to be prepared for pressure from the PEBLO to waive their right to a rebuttal so that they have an appropriate response ready.
Servicemembers or their representatives have only 5 days to submit the MEB rebuttal and request an impartial medical review. Extensions of time may be granted when good cause is shown. Therefore, it is important to review medical records in advance and consider documentation concerning any adverse or incorrect information in the records before the MEB report is completed.
Physical Evaluation Board (PEB)
The medical board report, any rebuttal, underlying medical records, the non-medical assessment and the line of duty investigation report, if any, are then forwarded to the service’s Central Physical Evaluation Board (CPEB) for non-hearing consideration by the IPEB. The PEB will sometimes return reports to the medical treatment facility if medical evaluation or appropriate testing was not conducted, or documents such as the non-medical assessment were not included. In addition, the MEB will sometimes submit an addendum if significant changes occurred since the initial medical board report was prepared. Medical information used to substantiate the existence or severity of unfitting conditions may not be more than 6 months old (DTM-11-015, p. 2). Note that requiring all medical evaluations to be performed by VA-certified physicians is meant to reduce the chance that MEB examinations and reports will be insufficient for meeting the needs of the PEB and the VA disability rating process.
IPEBs make findings and recommendations as to whether conditions result in medical unfitness, whether discharge or retirement is warranted, and whether conditions existed prior to entry or were the result of misconduct. They apply the previously-determined VA ratings to all conditions they find unfitting. Their findings and recommendations are terse, often presented without real explanation or rationale.
IPEB reports are then returned to the medical treatment facility and provided to the servicemembers along with further information about their rights from the PEBLOs. Findings and recommendations are considered final if members accept them at this point.
Request for Reconsideration
Members who disagree with a recommendation for discharge or retirement, or with the disability rating, may make a written request for reconsideration to the PEB. (DoD 1332.38, Encl. 3.3.3.4)
Formal PEB
If the written request for reconsideration of the IPEB is unsuccessful, members have the further right to a hearing before a FPEB. (DoD 1332.38, Encl. 3.1.3.3.1.1) Unfortunately, those found medically fit by IPEBs have no right to a FPEB (Encl. 3.1.3.3.1.2) or the remainder of the PEB process, though nothing prevents them from rebutting the IPEB or making a request for a FPEB. For these individuals, further medical evaluation and a new attempt at a medical evaluation board are often necessary, unless their cases show obvious abuse of discretion or lack any basis in fact, in which case resort to federal habeas corpus would be appropriate.
FPEBs provide the first and only opportunity for a hearing in the disability process. Traditionally held at major military hospitals, the Navy now holds its FPEBs in Washington, D.C. Members may be represented by attorney or non-attorney counsel, testify, and present witnesses and documentary evidence. Hearings are informal, but board members may be vigorous in questioning members. FPEBs are required to provide some justification of their decisions.
Representation at Formal PEB
Military attorneys are appointed to represent members prior to FPEB hearings. Some members choose to be represented by counselors from veterans service organizations such as the Disabled American Veterans (DAV). Civilian attorneys and counselors may provide representation.
In the Navy, at least, it is common for military attorneys to meet with clients for the first time on the day before the hearings, severely limiting preparation. Military counsel often have a good understanding of the decision-making patterns, biases and attitudes of board members. Perhaps as a result, some appointed attorneys tend to think that particular ratings for particular conditions are a forgone conclusion. Few have extensive experience in developing and presenting detailed medical and lay evidence, and the lack of time for advance preparation further limits this work.
Civilian advocates can play a key role prior to hearings by preparing members to testify, preparing any witnesses and developing additional evidence of the extent or severity of medical conditions, their impact on performance of duties, etc. Testimony or statements from lay witnesses, including fellow servicemembers, friends and family members, may be useful in arguing for increased disability ratings. Civilian medical evaluations can be used to challenge problems in MEB reports or IPEB findings.
Formal hearings offer important opportunities to provide evidence concerning pre-existence of medical conditions, service aggravation, and line of duty determinations. Well-prepared testimony from clients can have an important impact on the boards, as can the opportunity for board members to observe soldiers’ or sailors’ appearance or symptoms. Attorneys or counselors can also provide important representation at the hearings. Although formal rules of evidence do not apply, advocates can challenge inappropriate or harassing questions and note for the record improper considerations, failure to obtain necessary medical evidence, and the like. If necessary, they can remind board members of specific standards and presumptions applicable to individual cases, and can assist clients in summarizing the real impact of illnesses or injuries on their lives.
Nothing prevents IPEBs on reconsideration, or FPEBs, from making findings less favorable to members than the prior findings and recommendations, so that members take some risks in pursuing their cases, and are well advised to have legal assistance. Navy PEB liaison officers have told one of this article’s writers that the IPEB does not reduce findings on reconsideration. This may be common practice, but unfortunately is not stated in the regulations. FPEBs can and do reduce disability percentages or make other reduced findings and recommendations.
Appealing the Decision of the Formal PEB
Further written appeal through the disability evaluation system is available in all of the services, though the form varies considerably. While there are no further hearing rights, the member may still make written appeals to reviewers and, ultimately, the secretary of the service.
Petitioning the Board for Correction of Military Records
Members who do not feel their cases have been handled appropriately also have the option of petitioning the Board for Correction of Military/Naval Records (BCM/NR). Since this is a lengthy procedure, it does not provide much help for those whose immediate goal is discharge. But for those discharged without proper benefits, the BCMRs offer an important remedy. These boards can change the final determinations in medical disability cases, place medically discharged personnel on medical retirement, increase disability ratings, or change administrative or end-of-term-of service discharges to medical retirement.
Application to the BCMRs must be made within three years of the error or injustice at issue, defined as the date of discharge. However, late applications are frequently accepted if the Board finds it in the interests of justice to do so. The BCMRs will review the propriety of the disability evaluation proceedings as well as factual matters. Failure to afford members their full rights in the disability proceedings will not warrant correction of the record unless the BCMRs also find the change to be medically warranted.
Litigation
The IDES provides for an appellate review phase for service members to contest their respective Service’s DES’s disposition, but there are cases that make it to the Court of Federal Claims. In reviewing servicemembers’ claims, the Court of Federal Claims is “required to give substantial deference” to the findings of the IDES (Sieben v. United States, 108 Fed.Cl. 1, 5 (2012). Few cases result in the courts rebutting the findings, but there are instances when courts do rule in favor of servicemembers. See, e.g. Stuart v. United States, 108 Fed.Cl. 458 (2013) (concluding that the Army failed to follow its procedures regarding the plaintiff’s medical treatment, documentation of medical conditions, and discharge from active duty); Boyle v United States, 101 Fed.Cl. 592 (2011) (remanding the case to be processed through medical channels, rather than administrative, because the Army board failed to acknowledge the total behavioral transformation of the plaintiff after his second deployment to Iraq and diagnosis of PTSD).
Service Specific Information
Army
As of August 2013, nine Army installations provided legal assistance to soldiers undergoing the MEB and PEB process through the Office of Soldiers’ Counsel. The attorneys and paralegals are uniformed or civilian attorneys trained in this area and with the mission “…to provide zealous, ethical, and effective representation and advocacy throughout all phases of the Army’s physical disability evaluation system.” (U.S. Army JAG Corps, Office of Soldiers’ Counsel) The PEBLO at those installations will have contact information. (Forts Bragg, Drum, Eustis, Sam Houston, Hood, Lewis, Tripler, Carson and Alaska’s Richardson and Wainwright as well as Walter Reed Hospital.)
Deployment of Ill and Injured Servicemembers
During the Iraq and Afghanistan wars, servicemembers have often been deployed to combat areas despite illnesses or injuries which would otherwise result in limited duty and medical treatment, or medical discharge/retirement. Pressure to deploy troops affected military commanders and doctors in making decisions about deployment; particularly in the Army, commands commonly overrode medical recommendations that members not deploy. Here, as in other areas of military medical policy, public outrage and Congressional pressure led to policies which should result in more careful screening, and non-deployment of those with serious physical or psychological problems.
All Department of Defense (DoD) servicemembers must undergo a medical assessment prior to deployment that includes completion of DD Form 2795, a review of the servicemembers’ medical records, and a current Periodic Health Assessment (DoD Instruction 6490.07; see also DoD Instructions 6490.12 and 6490.03). DD 2795 must be completed within 120 days of deployment and reviewed in a face-to-face interview with a credentialed health care provider. The provider then makes a provisional determination of deployability.
Service members with pre-existing conditions may be deployed after a medical evaluation if certain conditions are met:
- The condition is not of such a nature or duration that an unexpected worsening or physical trauma is likely to have a grave medical outcome or negative impact on mission execution
- The condition is stable and reasonably anticipated by the pre-deployment medical evaluator not to worsen during the deployment in light of physical, physiological, psychological, and nutritional effects of the duties and location
- Any required, ongoing health care or medications anticipated to be needed for the duration of the deployment are available in theater within the Military Health System. Medication must have no special handling, storage, or other requirements (e.g., refrigeration, cold chain, or electrical power requirements). Medication must be well tolerated within harsh environmental conditions (e.g. heat or cold stress, sunlight) and should not cause significant side effects in the setting of moderate dehydration.
- There is no need for routine evacuation out of theater for continuing diagnostics or other evaluations.
DoDI 6490.07 lists eight categories of conditions which require a waiver for afflicted servicemembers to be considered deployable. The list is not all-inclusive; it states that additional factors to be considered when determining deployability include climate, altitude, rations, housing, duty assignment, and medical services available where the servicemembers will be stationed. Without a waiver, servicemembers shall not deploy with the following conditions:
- Conditions Affecting Force Health Protection: physical or psychological conditions resulting in the inability to effectively wear personal protective equipment and conditions that prohibit immunizations or the use of force health protection prescription products required for the specific deployment
- Unresolved Health Conditions Requiring Care or Affecting Performance: any chronic medical condition; absence of a dental exam within the last twelve months or likelihood that dental emergency will occur within twelve months; pregnancy; any medical condition requiring either durable medical equipment, or periodic treatment or evaluation not available where the service member is to be deployed; any unresolved acute or chronic illness; cancer requiring continuing treatment; precancerous lesions; any condition requiring surgery or a performed surgery that requires rehabilitation or additional surgery; musculoskeletal conditions; an acute exacerbation of a physical or mental condition that could significantly affect duty performance
- Conditions that Could Cause Sudden Incapacitation
- Pulmonary Disorders
- Infectious Disease
- Sensory Disorders: hearing loss (sufficient unaided hearing to perform duties) and vision loss
- Cardiac and Vascular Diseases: hypertension not controlled with medication or requiring frequent monitoring; symptomatic coronary artery disease; history of myocardial infarction within one year of deployment; history of coronary artery bypass graft, coronary artery angioplasty, carotid endarterectomy, other arterial stenting, or aneurysm repair within one year of deployment; cardiac dysrhythmias or arrhythmias, either symptomatic or requiring medical or electrophysiologic control (presence of an implanted defibrillator and/or pacemaker); heart failure
- Mental Health Disorders: psychotic and/or bipolar disorders; psychiatric disorders under treatment with fewer than three months of demonstrated stability; clinical psychiatric disorders with residual symptoms; conditions that pose a substantial risk for deterioration and/or recurrence during deployment; chronic conditions that require ongoing treatment with antipsychotics, lithium, or anticonvulsants.
Waiver requests are to be submitted to the applicable Combatant Commander through the members’ servicing military medical unit, with medical input provided by the individuals’ medical provider. The waiver must include a summary of the detailed medical evaluation of the condition and be justified with “statements indicating service experience, position to be placed in, any known specific hazards of the position, anticipated availability and need for care while deployed, the benefit expected to accrue from the waiver, [and] the recommendation of the commander or supervisor” (DoD Instruction 6490.07).
All deploying servicemembers are required to complete a person-to-person pre-deployment mental health assessment and three post-deployment mental health assessments. Deployment limitations associated with mental health conditions are those that are not “amenable or anticipated not amenable to treatment and restoration to full functioning within one year of onset of treatment” (Policy Guidance for Deployment-Limiting Psychiatric Conditions and Medications, DoD Policy Memo (November 7, 2006)). Servicemembers with conditions falling under these criteria should be referred to the disability evaluation system for Medical Evaluation Boards and possible discharge or retirement. Conditions not meeting the threshold to be referred to the MEB should display a pattern of stability without significant symptoms for at least three months prior to deployment. Psychotic and bipolar disorders, however, are considered disqualifying for deployment, while those with psychotic conditions in remission or not impairing duty performance may be considered deployable. Whether a condition will deteriorate or symptoms will recur during deployment, considering environmental and mission demands, must also be considered in determining deployability. While deployed, the clinical decision to retain servicemembers is based on the severity of symptoms and/or medication side effects; degree of functional impairment; risk of exacerbation if members were exposed to trauma or severe operational stress; ability of the members to psychologically tolerate the rigors of deployment; and prognosis for recovery.
The Department of Defense has also implemented a policy to treat psychological injuries similarly to other physical injuries with a “psychological first aid” program of prevention and protection. DoD Instruction 6490.05 states that “psychological interventions for combat and operational stress reactions shall be implemented by first-responders on the same parity with physical injuries in order to mitigate the risk of potential longer-term physical and psychological consequences of combat and other military operations.” Additionally, it is Department policy that emergency mental health evaluations are required for servicemembers whenever they intend or are likely to cause serious injury to themselves or others, or when a commanding officer believes that members may be suffering from a severe mental disorder (DoDI 6490.04, Mental Health Evaluations of Members of the Military Services (March 4, 2013).
The Department of Defense’s policy for deployment-limiting conditions is extensive; however, much of the process is discretionary and there is not always a bright line distinction between conditions that make servicemembers deployable and those that do not.
Conclusion
The very conditions for which people seek medical help or discharge/retirement may affect their ability to achieve it. Accordingly, these proceedings, and medical discharges generally, are important areas for counseling and advocacy. Clients who have the assistance of advocates or simply have full explanations of the medical standards and their rights are likely to fare much better than others in obtaining treatment and in the disability evaluation system. This is particularly true when debilitating effects of combat impair clients’ ability to navigate the system while their symptoms are acute, and the disability process itself causes additional stress. As the current wars progress and increasing numbers of soldiers try to cope with illness and injury, those who face doctors and disability proceedings alone often find their conditions undiagnosed or under-diagnosed and their rights neglected.
The Task Force encourages counselors and attorneys to educate themselves in this area and to include military disability cases in their work.
This memo, originally written by Kathleen Gilberd and Luke Hiken, was revised and updated in January, 2014, by Alison Carter, Kathleen Gilberd, Jeff Matus, and Katie Tastrom, with helpful comments from Kit Anderton and Lenore Yarger.

{kind=link}